Authored by:
Greg Vigna, MD JD; Adam Suchecki, Orthopedic PA, CLCP;
Vanessa Young, OTR/L, CLCP; Elizabeth German, DPT
Introduction:
The calcaneus, commonly known as the heel bone, is part of the hindfoot and is the largest and most frequently fractured of the tarsal bones. Calcaneal fractures account for 2% of all fractures among the adult population (4, 10, 11). “The annual incidence of calcaneal fractures is approximately 11.5 per 100,000 individuals” (7). To fully understand the significance of a calcaneal fracture, one must first understand its anatomy and function.
The tarsal bones consist of seven bones in the ankle and heel. Together, they support body weight, enable movement while providing stability during ambulation, and function as shock absorbers during walking, running, jumping, and other activities (7). The articulation between the calcaneus and talus is known as the subtalar joint. This joint primarily facilitates inversion and eversion. However, it also contributes to motion at the ankle joint itself, formed by the talus, tibia, and fibula, by assisting with dorsiflexion and plantarflexion (11).
The calcaneus plays a crucial role in weight-bearing activities. It accepts body weight from the initial heel contact and continues through midstance during ambulation (21). It also has four articular surfaces, allowing it to interact with surrounding bones and provide multiple sites for smooth movement. As noted in the literature, “Due to its complex anatomy – being the largest tarsal bone and having an articular component – the majority of the axial load of the body weight affects the calcaneus. Therefore, injuries lead to changes in the mechanics and function of the foot, which can lead to impairment” (4).
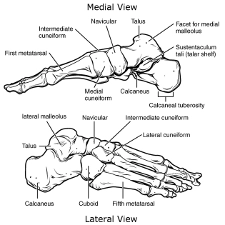
(24)
Calcaneal fractures are complex, and a consistent fracture pattern is less common than in other fracture sites. Fracture patterns are influenced by several factors, including the shape and position of the talus and calcaneus, the internal structure of the calcaneus (particularly the distribution of trabecular bone), and the magnitude and duration of the traumatic force (1).
Historically, calcaneal fractures were referred to as a “lover’s fracture,” based on the idea that they occurred when a suitor jumped from a lover’s balcony to avoid detection (6). Over time, both the naming and classification of these fractures have evolved. Currently, calcaneal fractures are generally divided into two categories:
Several naming classifications have been used over the years to describe calcaneal fractures. “In the last five decades, 49 classification systems of calcaneal fractures have been proposed, and 19 of them are considered current” (3). Some of the more widely recognized classification systems are the Orthopaedic Trauma Association (OTA) Classification; Crosby; Rammelts and Zwipp; Goldzak; Bohler; Essex-Lopresti; and Sanders.
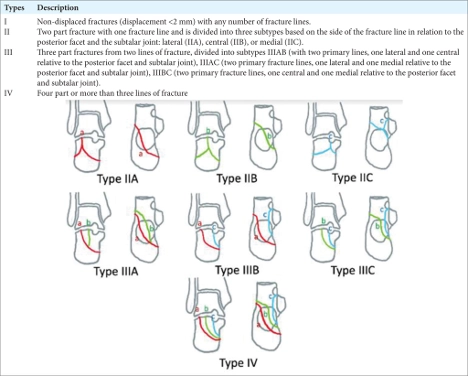
The most commonly used classification system is the Sanders Classification. This CT (computed tomography) scan based classification, grades the intra-articular displacement of the posterior facet, thus classifying the injury into 4 major types depending on the number of fracture lines (in essence, the number of separated parts). “Although Sanders classification is the most used system for classifying displaced intra-articular calcaneal fractures (DIACFs) over the world, the assessment of this classification was fair in all published studies and its usefulness (especially the subtypes A, B, and C) has been questioned.” (3) See below:
(25)
Calcaneal fractures are known to significantly impact patients’ lives, and can lead to physical, mental, social and occupational challenges. “Regardless of treatment, calcaneal fractures are associated with numerous complications and poor prognosis with significant long-term quality-of-life issues”. (1)
Forces Causing Injury:
Calcaneal fractures occur most frequently in young, active males between 30 and 50 years of age. They typically result from high-energy axial loading, in which force drives the talus downward into the calcaneus (2, 4, 6, 7, 11). For example, “falls from a height directly translate energy into the calcaneus on impact as the heel strikes a surface crushing the calcaneus against the talus. The talus acts as a wedge and causes depression and the widening of the calcaneal body” (6, 7). The primary causes of calcaneal fractures include falls from height, motor vehicle accidents, slip-and-fall injuries, sports-related trauma, and crush injuries. The resulting fracture pattern depends on the direction and intensity of the force, the position of the foot at the time of injury, and the patient’s bone quality (2).
Patient Presentation (Symptoms and Physical Findings):
Oftentimes, patients with calcaneal fractures have sustained this injury as a result of high energy force. For this reason, a thorough and comprehensive examination is essential. In trauma specific patients, assessment should begin with the ATLS (Advanced Trauma Life Support) algorithm. Once stabilized, the clinician should focus their assessment on the foot and lower leg. The assessment should include evaluation for pain and deformities of the hindfoot, midfoot and forefoot, along with assessment for skin lesions, sensory deficits, distal pulses, tendon function in the lower extremities and overall perfusion. Importantly, an early comprehension evaluation can increase the likelihood of early detection of complications such as compartment syndrome.
Common clinical findings in patients with calcaneal fractures typically include: pain; plantar ecchymosis (Mondor’s sign); significant edema; hindfoot deformity, and impaired function and or difficulty bearing weight. Lastly, the evaluation of soft tissue integrity is essential, as it can influence surgical planning.
Calcaneal fractures are often associated with concomitant injuries due to their high-energy origin. Clinicians must consider the possibility of bilateral calcaneal fractures, particularly in cases involving falls where the individual lands on both feet. It is important clinicians also assess for injuries that may have occurred throughout the lower extremities, as well as into the spine, abdomen, and thoracic structures, due to the high forces transmitted during injury. Common co-occurring fracture sites include tibial plafond (roof of ankle joint), tibial plateau, spine, femur, and pelvis (2, 4).
Diagnostic Testing:
Radiographs are the primary imaging modality for calcaneal fractures. Standard views include lateral, anteroposterior, and oblique foot radiographs, along with axial views of the calcaneus (2). The radiologist will evaluate Bohler’s and Gissane’s angles, and compare them to normative data. Bohler’s angle is the angle on the lateral foot radiograph between a line joining the highest point of the anterior process of the calcaneus and the highest point of the posterior articular facet, and a line joining the highest point of the posterior articular facet with the highest point of the calcaneal tuberosity[1]. The Gissane angle is measured by drawing lines along the superior surface of the anterior process and the posterior facet of the calcaneus to meet at the calcaneal sulcus which is the top of the calcaneus. Computed tomography (CT) further enhances fracture diagnosis, classification and prognosis. “CT reconstructions allow better comprehension of the fracture anatomy, helping with the surgical planning, with possible reduction maneuvers, and fixation choices” (2). Magnetic resonance imaging (MRIs), although less commonly used, may aid in the diagnosis of occult or pathological fractures and in identifying soft-tissue injuries.
Surgical and Non-Surgical Treatment:
Optimal management and treatment of calcaneal fractures has been controversial over the years. Understanding the indications for surgical versus conservative treatment is essential, and the treating physician must carefully weigh the risks and benefits of each choice. As defined by the American Orthopedic Foot and Ankle Society (AOFAS), “The goal of calcaneal fracture treatment is to restore the normal alignment and contour of the calcaneus. This is achieved by restoring heel height and length, the realignment of the posterior facet of the subtalar joint, and restoring the mechanical axis of the foot” (9).
Surgical interventions may improve functional outcomes by restoring calcaneal morphology and joint articular congruency. However, it has also been associated with higher risk of complications, particularly soft tissue problems, infections and wound dehiscence (4, 6, 11). Regardless of whether treatment is surgical or non-surgical, initial management should include wound care and antibiotics when needed, analgesics, ice and elevation, immobilization or splinting (such as a Bulky Jones Splint); and strict non-weight bearing of the injured lower extremity.
When considering surgical management, “the literature demonstrates that anatomical reduction and internal fixation provide the best outcomes in terms of rapid recovery and early restoration of subtalar joint function. The gold standard in treatment should include anatomical reduction of the subtalar joint, restoration of the normal width, alignment, and length of the calcaneus, and stabilization with rigid fixation.” (2, 5)
Primary indications for surgical intervention include: (7, 9)
Surgical approaches for calcaneal fractures include both open reduction internal fixation (ORIF) and percutaneous fixation. Two commonly used ORIF approaches are the extended lateral approach, and the less invasive sinus tarsi approach. The sinus tarsi approach has been shown to provide comparable functional outcomes to the extended lateral approach, while reducing soft tissue complications (2). Percutaneous options include both a percutaneous screw fixation and external fixation. These techniques aim to reduce the risks associated with open surgery while still providing stabilization and supporting anatomic reduction of the calcaneus.
When the surgical risks outweigh the potential benefits, calcaneal fractures are managed conservatively. Conservative treatment is typically indicated in the following situations (11)
Conservative management generally begins with rest, ice, analgesics, minimized weight bearing, and immobilization, often using a bulky Jones splint and an assistive device for mobility. Once swelling subsides, the splint is typically converted to a well-padded cast, with a total non-weight bearing period of approximately 10 to 12 weeks post-injury. After healing is confirmed, the patient may begin gradual progression of weight bearing and participate in therapy, based on physician recommendations.
Rehabilitation Required:
Calcaneal fracture patterns vary greatly, and rehabilitation protocol should be individualized to optimize functional outcomes. A physical therapist will assist in guiding the patient through the recovery process. Rehabilitation is typically tailored based on the type and severity of the fracture, the treatment approach and protocol established by the treating orthopedic physician, and the patient’s initial functional status and personal goals.
Physical therapy for calcaneal fractures generally follows consistent principles and phases of recovery, with varying degrees of implementation based on injury and clinical discretion. The phases include:
Home Modifications:
Following injury to the calcaneus, whether managed surgically or non-surgically, adjustments to the home environment are often necessary. In the early recovery phase, these changes promote safety, reduce fall risk, and make daily activities more manageable. Over the long term, home modifications can also support independence if pain, mobility limitations, or additional surgeries arise. A meta-analysis by Stark, Keglovits, Arbesman, and Lieberman (2017) found strong evidence that home modification interventions improve function and reduce both the rate and risk of falls in community dwelling adults. (23)
Postoperative/Short-Term Modifications:
Short-term needs focus on supporting reduced weight-bearing, maintaining participation in ADLs (activities of daily living), and preventing re-injury. Bathroom safety can be addressed with the use of a shower chair, grab bars, a handheld shower head, and, when needed, a raised toilet seat with arms, along with appropriate wound protection during bathing. Adaptive equipment may include, depending on the individual, a bedside commode, item carriers, and mobility aids such as a wheelchair, knee scooter, walker, or crutches. Immobilization and stability devices, such as a bulky Jones splint (11), a CAM boot, or other post-operative braces, should also be considered. Client-centered modifications may involve temporary portable ramps or threshold adjustments, additional grab bars and handrails, and the option to set up living space on one floor. Depending on the client’s age, strength, home set-up, and family dynamics, a temporary caregiver may be necessary for things such as meal preparation, driving, grocery acquisition, and deep cleaning.
Long-Term Modifications
If a patient experiences long-term complications such as osteoarthritis, nonunion, or malunion, permanent modifications may be needed to promote safety, independence, and mobility. These may include fixed grab bars in high-use areas, raised laundry baskets to reduce bending demands, anti-fatigue mats to improve comfort during prolonged standing, and supportive footwear to reduce joint stress and enhance stability.
Community mobility devices, such as a power scooter with a lift, may become necessary with advancing age or declining endurance. Seating arrangements such as recliners, with or without lift functions, may assist with edema management, transfers, and overall independence as mobility changes over time.
Lifestyle modifications should be considered for optimal function and patient satisfaction long-term. (7) These modifications could include any, or all, of the following:
Early Complications:
Complications are relatively common with calcaneal injuries. “The reported complication rates after ORIF vary widely in the literature, ranging from 10-40% depending on the surgical technique, patient characteristics, and injury severity” (4). Complications that are more specifically associated with surgical repair include sural nerve injury, infection, wound healing problems (suture dehiscence), hardware complications (such as loosening, migration, or irritation), and neurovascular compromise (7).
Additional complications may occur with or without surgical intervention, including chronic pain, stiffness (loss of subtalar mobility), gait abnormalities, neurological injury, and fibular tendonitis (2, 5, 6).
Future Complications:
With any calcaneal fracture injury, one must be cognizant of the development of nonunions, malunions, post-traumatic osteoarthritis, osteomyelitis or complex regional pain syndrome (11).
As reviewed earlier, the calcaneus forms multiple joint articulations and serves as a primary weight-bearing structure. Because of this, injuries that alter the mechanics and/or function of the foot can quickly lead to impairment (13). Over time, surface incongruity at the subtalar joint is a primary contributor to the development of post-traumatic osteoarthritis in these patients. Similarly, malunion can have significant long-term consequences. As noted in the literature, “once a severe calcaneal malunion causes the disorder of the motion axis from the hindfoot to the whole lower limb, this will result in an abnormal gait with symptoms and dysfunction of the joints and muscles, eventually leading to pain and permanent disability. Thus, calcaneal malunion may be life-altering to patients, not only because it imposes a great symptomatic effect but also because it carries a huge economic burden” (22). Non-specific lower back pain has long been linked and generally accepted in the medical community associated with deviations in gait related to podiatric dysfunction.[2]
In summary, although (generally) not life threatening, calcaneal injuries may still result in permanent disability. (12) “With the average age of 40 years (at injury)…as this represents the working-age population, calcaneal fractures in this age group can lead to prolonged occupational disability with a significant socioeconomic impact” (4). Prompt and appropriate treatment of calcaneal injuries is of paramount importance, as “neglected or improperly managed calcaneal fractures can lead to persistent pain, altered gait, and long-term disability” (7).
Patient Profile:
A 38-year-old male construction worker sustained an injury to his left heel after falling approximately 10 feet from scaffolding, landing directly on his feet. He immediately experienced severe heel pain and swelling, with an inability to bear weight on the affected limb. The patient presented to the emergency department within one hour of injury, reporting diffuse pain localized to the posterior heel and hindfoot, and mild numbness along the lateral aspect of the foot. The patient denied loss of consciousness or other major injuries. He described a “crunching” sensation at the moment of impact, followed by rapid onset of swelling and bruising over the heel. There was no open wound or visible deformity, but significant tenderness was noted over the calcaneal tuberosity and lateral hindfoot.
Inspection revealed marked edema and ecchymosis extending from the medial to lateral heel, with a positive “Mondor sign” (plantar ecchymosis) indicating potential intra-articular involvement. Palpation elicited sharp tenderness over the posterior calcaneus and subtalar region. The patient was unable to perform active plantar flexion due to pain. The ankle joint was grossly stable, and distal pulses were intact. Sensation was preserved throughout the foot. Plain radiographs (lateral, axial, and oblique views) demonstrated loss of Böhler’s angle and depression of the posterior facet of the calcaneus, consistent with a displaced intra-articular calcaneal fracture. A computed tomography (CT) scan confirmed a Sanders Type II fracture, involving the posterior facet with displacement greater than 2 mm, but no comminution of the sustentaculum tali.
Initial management included limb elevation, posterior splint immobilization, and administration of intravenous analgesics and ice therapy to control swelling. The patient was advised strict non-weightbearing on the affected extremity. After resolution of soft tissue edema (confirmed by skin wrinkling at 7 days post-injury), open reduction and internal fixation (ORIF) via an extensile lateral approach was performed. An anatomic reduction of the posterior facet was achieved and stabilized with a low-profile calcaneal plate and screws. Intraoperative fluoroscopy confirmed restoration of Böhler’s and Gissane’s angles.
The patient remained non-weightbearing for 10 weeks in a short leg splint, progressing to partial weightbearing in a controlled ankle motion (CAM) boot. Deep vein thrombosis (DVT) prophylaxis was maintained during immobilization. Physical therapy began at 8 weeks, focusing on ankle and subtalar joint range of motion, peroneal muscle strengthening, and gradual gait retraining. At 12 weeks postoperatively, radiographs showed satisfactory fracture healing and hardware integrity. The patient transitioned to full weightbearing at 14 weeks. At 6 months, he demonstrated near-normal gait and subtalar mobility with mild stiffness during uneven terrain ambulation. He reported intermittent discomfort after prolonged standing but had returned to modified work duties. At the 1-year follow-up, the patient exhibited solid union, pain-free gait, and full return to work. He was counseled regarding the potential for late subtalar arthritis and advised periodic follow-up for monitoring.
Life Care Plan Considerations:
Note: Each surgical procedure comes with: preoperative clearance visit, post-operative pain medications, possible blood thinners (if indicated), post-operative outpatient physical therapy, home health considerations for PT/OT/RN in acute healing phase (if indicated), attendant care for 2-6 weeks depending on procedure (if indicated), bracing/orthotic needs, and DME. Surgical considerations for advanced subtalar joint OA include:
Injury Care Solutions Group (ICSG) provides educational expert content that does not constitute medical advice, diagnosis, treatment, or legal advice or solicitation. ICSG is not a law firm or medical provider. Use of this website does not create a doctor–patient or attorney–client relationship. Do not send PHI through this Website. Attorney references (including references to Ben Martin Law Group) are for convenience only, and are not endorsements, guarantees or attorney advertising. Past results do not predict future outcomes. See Full Disclaimer and Privacy Policy. If deemed attorney advertising: Ben C. Martin, 4500 Maple Ave., Suite 400, Dallas, Texas 75219, licensed by the State Bar of Texas and Pennsylvania.