Authored by:
Greg Vigna, MD; JD; Adam Suchecki, Orthopedic PA, CLCP;
Vanessa Young, OTR/L, CLCP; Elizabeth German, DPT
Introduction: Jones (5th Metatarsal) Fracture
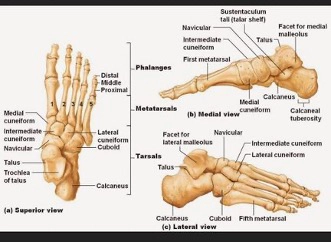
Metatarsal fractures are the most common injury of the foot, accounting for 35% of all foot fractures. (3) And of these, 45-70% involve the fifth metatarsal. (1) The fifth metatarsal is located on the most lateral border of the forefoot. This bone consists of the head, shaft, and base. The proximal aspect of the fifth metatarsal is known as the base and articulates with both the cuboid bone and the base of the fourth metatarsal. Structures that specifically attach to the base of the fifth metatarsal include the: peroneus brevis tendon, peroneus tertius tendon, abductor digiti minimi, and lateral band of the plantar fascia ligament. (1) The proximal aspect of the fifth metatarsal is relatively fixed with movements, due to strong ligament attachments with the cuboid and other metatarsal bones. The distal end of the fifth metatarsal is, however, more mobile. (1) The fifth metatarsal works alongside the fourth, to play a pivotal role in foot mechanics by facilitating weight distribution and acting as a shock absorber on uneven surfaces with gait. (5) It allows considerably more movement than the remaining metatarsals, at 13mm in the sagittal plane. (20)
(21)
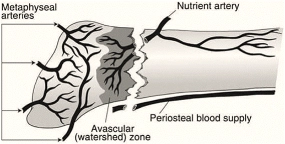
There is considerable research regarding fractures of the fifth metatarsal, which may be due to the increased risk of poor healing (delayed healing, nonunion, or malunion) associated with these fractures. One reason this occurs is due to the unique blood supply surrounding the base of the fifth metatarsal. Blood supply at the base is derived from 3 sources: the nutrient artery, the metaphyseal artery, and the periosteal artery. A watershed area (area of decreased blood supply) exists between the blood supply of the metaphyseal artery perforators and the retrograde branches of the nutrient artery. (2) This watershed area is known to be the most likely location of poor fracture healing that occurs at the base of the fifth. (7)
(9)
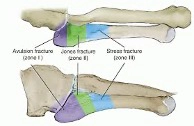
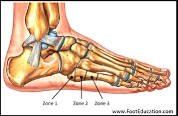
Fifth metatarsal fractures are typically referred to as Jones fractures, although this nomenclature isn’t as clear-cut as it seems. “In the literature different definitions of ‘Jones fractures’ were developed…due to different terminology, there is no standardized treatment recommendation for all fracture types of the proximal fifth metatarsal bone”. (2) Over the years, various classification systems have emerged to name fifth metatarsal fractures. Currently, the Lawrence and Botte classification is the most commonly used among physicians and separates the base of the fifth into 3 zones. (2)
There is no one treatment option for all fractures to the base of the fifth metatarsal, and knowing this, reinforces the crucial nature of correctly diagnosing and classifying metatarsal fractures in order to make optimal treatment and individualized management decisions.
(23)
(22)
Forces Causing Injury:
Metatarsal injuries in the foot frequently result from low-energy trauma (in about 85% of cases). (3) With fractures occurring at the base of the fifth metatarsal, it is important to note that differing forces cause injuries to different zones.
The risk of stress fractures occurring is increased with prior history of stress fractures, recent intense/change in activity level, osteopenia, and endocrinopathies. (1)
Patient Presentation (Symptoms and Physical Findings):
Differentiating between acute fractures or stress fractures is important for the physician to initially determine. With acute fractures, there is generally localized swelling and tenderness, difficulty walking/weight bearing, and ecchymosis. With stress fractures, pain usually occurs in the prodromal phase and is often present for several weeks before a patient seeks medical treatment. (1)
The patient may present to their physician with complaints of pain including:
Diagnostic Testing:
If a physician determines there is a need for further testing past their clinical examination, they may order standard 3 view radiographs of the foot and ankle, including an anterioposterior, lateral and oblique view radiograph. To note, stress fractures are usually absent in the early stages on radiograph and may require repeat radiographs after 10-15 days. (7)
Additional testing that may assist in accurately diagnosing fractures of the fifth metatarsal include:
Surgical and Non-Surgical Treatment of Jones Fractures:
Recommendations as to treatment of Jones Fractures should be individualized and determined based on the fracture type & location, associated injuries, individual patient characteristics, and the patient’s fitness & activity levels. (10) Fractures in various zones in the base have been shown to heal and recover at various rates. “Fractures of the greater tuberosity both at a proximal and distal level have the propensity to heal given the numerous randomly distributed metaphyseal arteries. In contrast, fractures at the proximal metaphysis disrupt the nutrient artery, and hence create the so-called ‘avascular region’. Considerations of fracture location and potential vascular compromise should therefore always be taken into account and considered in the treatment strategy”. (1)
Non-operative, conservative, treatment for fractures at the base of the fifth metatarsal include: elastic bandage support, non-weightbearing casting, a hard-soled shoe for support, short-leg walking casts or CAM walker boots. (1) Prolonged immobilization is a hallmark of conservative treatment in this case. (12) A newer option for non-operative treatment may include using platelet rich plasma (PRP) injections, however there are few studies to date on the efficacy of this treatment. (12)
Surgical treatment options vary based on type and location of injury and may include intramedullary screw fixation (with or without bone grafting), tension band constructs, low-profile plate & screw fixation, percutaneous pinning, cerclage/external fixation, and closed reduction & cross pinning with K-wire fixation. In the case of nonunion, decortication and repermeabilization and aspiration of the medullary canal and freshening and bone grafting may be required. (1) With internal fixation, orthobiologics may be utilized as an adjunct therapy in treatment (for example BMAC). Typically, “surgical treatment is recommended for high-level athletes due to its association with a significant earlier return to play and lower rates of non-union”. (10)
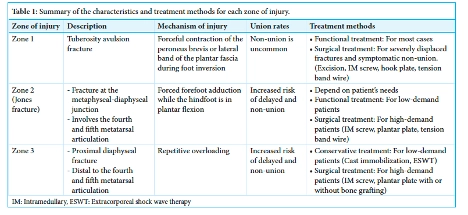
Treatment strategies are best outlined using the Lawrence and Botte classification of fractures. “Zone one, zone two and zone three fractures account for 93%, 4% and 3% of proximal fifth metatarsal fractures, respectively”. (7)
Zone 1 fractures are the non-displaced and displaced tuberosity avulsion fractures. In this region, non-operative treatment is widely recommended. “There is a general agreement that all non-displaced or minimally displaced tuberosity avulsion fractures should be treated conservatively”. (1) Although if there is a large fracture or bone fragment in this region it may require ORIF, closed reduction, percutaneous pinning, or excision of the fragment. (8)
Zone 2 fractures, the ‘Jones fractures’, are controversial in terms of optimal treatment. According to research performed by Ancelin, it is believed that zone 1 and zone 2 show similar behavior and may be treated identically. (3) According to a study by Baumbach et al. it was found that “When comparing Lawrence and Botte type 1 and 2 fractures no significant difference could be detected for any outcome parameter within a follow-up of 22+/-10 months… Type 2 fractures can be treated functionally with an excellent clinical outcome, comparable to Lawrence and Botte type 1”. (4) Alternatively, if the patient happens to need to return to high-level activity, numerous articles show acute Jones fractures treated operatively result in quicker return to sport and clinical healing in competitive athletes. (7)
Zone 3 fractures tend to lean toward surgical treatment options. This is due to the fact that “zone 3 fractures show high rates of delayed healing and non-union at 25-67%, and of re-fracture, at 50%, in patients managed by immobilization or functional treatment rather than surgery”. (3) It is possible to consider and trial conservative treatment, with a non-weightbearing cast, but the patient may need up to 20 weeks before radiographic union is seen with this route. (8) Because of this, it is generally believed that surgical intervention is significantly superior to non-operative treatment in many cases with zone 3 fractures. (3)
(10)
“Although controversy persists, the current trend in orthopedic care has been to treat non-displaced zone 1 fractures conservative, significantly displaced zone 1 fractures surgically, and zone 2 and 3 fractures either conservatively or surgically, depending on the overall patient expectations and activity level”. (13)
A recent study involving NFL players who suffered Jones Fractures indicate that nine weeks appears to be the optimum time to allow for union and allow for return to play is nine weeks as there is a statistically increased risk of need for requiring a second surgery if return to play is before nine weeks. (24) “Several systematic reviews conclude that surgery results in shorter union times and lower number of delayed union or non-unions”. (1)
Rehabilitation Required:
Since there are many presentations of fifth metatarsal injuries, rehabilitation must be individualized to optimize patient outcomes. A physical therapist will assist in guiding the patient through the recovery process. There is not one set protocol, but instead the rehabilitation process will be tailored by: the type/severity of fracture, the treatment approach and protocol of the orthopedic physician treating the patient, and the patient’s initial status and goals. (8)
Physical therapy generally follows similar principles and phases for recovery, with varying degrees of implementation based on injury and clinical discretion. The phases include:
Home Modifications:
Following a fifth metatarsal fracture, depending on location, and especially if requiring surgical intervention, adjustments in the home environment are often necessary. In the early recovery phase, these changes help ensure safety, reduce the risk of falls, and make daily activities more manageable. Over the long term, modifications can also support independence in the case that pain, dysfunctions of mobility, or additional surgeries occur. A meta-analysis by Stark, Keglovits, Arbesman, and Lieberman (2017) found strong evidence that home modification interventions improve function and reduce both the rate and risk of falls in community dwelling adults.
Postoperative Modifications:
Short-term needs include supporting reduced weight-bearing, maintaining ADL participation, and preventing re-injury. Mobility devices could include, knee scooter, crutches, walker, cane, CAM boot, and post-operative brace/s. Bathroom safety can be addressed with a shower chair, handheld shower head, raised toilet seat with arms, and wound protection. Adaptive equipment may include a bedside commode, item carriers, and mobility aids such as knee scooters, walkers, or crutches. Client-centered modifications may involve portable ramps or threshold adjustments, grab bars and handrails, and the option to set up living space on one floor or install a stair lift.
Long-Term Modifications
If a patient experiences long-term complications such as nonunion or malunion, permanent changes should be considered to promote safety, independence, and mobility. These may include fixed grab bars in high-use areas, raised laundry baskets, anti-fatigue mats for prolonged standing, and supportive footwear to reduce joint stress. Community mobility devices, such as a power scooter with lift may be necessary as one ages. Adjustable beds can aid rest and assist with leg elevation, while recliners with or without lift functions support edema management, transfers, and independence as mobility declines with age.
Early Complications:
If the initial injury involves open skin, one must assess for skin infection during healing. With either surgical or conservative treatment options, if the patient is not showing signs of healing in 6-8 weeks (absence of callus formation), it would be crucial to consider trialing pulsed electromagnetic field therapy. (1) This is a non-invasive adjunct therapy that can be used to assist in treating delayed unions or stimulate bone growth. It can be performed via low-intensity pulsed ultrasound (LIPUS) or extracorporeal shock wave therapy (ESWT). (10)
“Whether to treat metatarsal fractures conservatively or surgically is controversial; surgical intervention may reduce the incidence of nonunion, but the complication rate of surgery can be high”. (6) Surgical complications could include hardware failure, prominence of the screwhead, wound infection/delayed wound healing, donor site morbidity (with bone grafting procedures), refracture, Sural nerve injury, malunion, or delayed union/nonunion. To note, nonunion in the literature is “characterized by the failure of a fracture to heal within a prolonged period, typically beyond nine months, with no evidence of healing progression for at least three months”. (5)
Future Complications:
Long term complications seen with fractures at the base of the fifth metatarsal include: refracture, chronic low-level pain, iatrogenic fractures, malunion or delayed union/nonunion. Surgical correction of nonunion or malunions may be necessary. Osteoarthritis in the surrounding joints may occur, and its incidence depends on the initial damage and quality of the reduction. (3)
Fractures at the base of the fifth metatarsal are relatively common in terms of fractures of the foot, however their treatment can be complicated. One must have a thorough understanding of the anatomy and location of the injury, forces that caused the injury, and treatment options, both conservative and surgical. Healing of the fracture is often tracked radiographically due to the risk of nonunion, malunion or delayed healing. Physical therapists are utilized to improve healing and return the patient to functional activities. Understanding the nature of these fractures and following the correct treatment protocols results in the most optimal patient outcomes. Future care for Jones fractures relates to injuries to the CMC joint, risk of post-traumatic arthritis, and associated injuries. Future treatments may include orthopedic follow up, removal of hardware, modalities, diagnostic, pain management, and orthotics.
1. Chloros, G. D., Kakos, C. D., Tastsidis, I. K., Giannoudis, V. P., Panteli, M., & Giannoudis, P. V. (2021). Fifth metatarsal fractures: An update on management, complications, and outcomes. EFORT Open Reviews, 7(1), 13–25. https://doi.org/10.1530/EOR-21-0025
2. Pfüger, P., Zyskowski, M., Müller, M., Kirchhof, C., Biberthaler, P., & Crönlein, M. (2021). Functional outcome of 103 fractures of the proximal fifth metatarsal bone. European Journal of Medical Research, 26(1), 150. https://doi.org/10.1186/s40001-021-00623-6
3. Ancelin, D. (2025). Metatarsal fracture without Lisfranc injury. Orthopaedics & Traumatology: Surgery & Research, 111, 104059. https://doi.org/10.1016/j.otsr.2024.104059
4. Baumbach, S. F., Prall, W. C., Kramer, M., Braunstein, M., Böcker, W., & Polzer, H. (2017). Functional treatment for fractures to the base of the 5th metatarsal – Influence of fracture location and fracture characteristics. BMC Musculoskeletal Disorders, 18, 534. https://doi.org/10.1186/s12891-017-1893-6
5. Hill, Z., Cao, C., Pookun, P., Ebanculla, F.J., & Chen, G. (2025). Surgical excision of symptomatic nonunions of the fifth metatarsal base fractures: a systematic review of outcomes and complications. Foot & Ankle Surgery: Techniques, Reports & Cases, 5. https://doi.org/10.1016/j.fastrc.2025.100514
6. Nolte, P., Anderson, R., Strauss, E., Wang, Z., Hu, L., Xu, Z., & Steen, R. G. (2016). Heal rate of metatarsal fractures: A propensity-matching study of patients treated with low-intensity pulsed ultrasound (LIPUS) vs. surgical and other treatments. Injury, 47(12), 2584–2590. https://doi.org/10.1016/j.injury.2016.09.023
7. Bowes, J., & Buckley, R. (2016). Fifth metatarsal fractures and current treatment. World Journal of Orthopedics, 7(12), 793–800. https://doi.org/10.5312/wjo.v7.i12.793
8. Smidt, K. P., & Massey, P. (2023). 5th metatarsal fracture. In StatPearls [Internet]. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK544369/
9. Gawhale, S., Gohil, K., Ghag, N. S., & Chavan, K. S. (2025). Optimizing stability and healing in Jones fracture nonunion: A novel approach of fixation. Journal of Orthopaedic Reports, 4, 100389. https://doi.org/10.1016/j.jorep.2024.100389
10. Eldessouky, A., & Bhatia, M. (2025). Fifth metatarsal fractures: Review of the current concepts. Journal of Arthroscopic Surgery and Sports Medicine, 6(1), 24–31. https://doi.org/10.25259/JASSM_34_2024
11. Barnds, B., Heenan, M., Ayres, J., Tarakemeh, A., Schroeppel, J. P., Mullen, S., & Vopat, B. G. (2021). Comparison of the rate of delayed/nonunion in fifth metatarsal fractures receiving anti-inflammatory medications. Journal of Experimental Orthopaedics, 8, 115. https://doi.org/10.1186/s40634-021-00435-x
12. Luo, E. J., Anastasio, A. T., Stauffer, T., Grant, C., Wu, C. J., Wu, K. A., Kaplan, S., & Lau, B. C. (2024). Jones fracture in the National Football League. Sports, 12(1), 7. https://doi.org/10.3390/sports12010007
13. Kim, C., Shin, D. Y., & Kim, J. (2024). Is surgical treatment necessary for the treatment of a Jones fracture? A retrospective study. Clinics in Orthopedic Surgery, 16(2), 335–341. https://doi.org/10.4055/cios23333
14. Quill, G. E., Jr. (1995). Fractures of the proximal fifth metatarsal. Controversies in Foot and Ankle Trauma, 20, 353–361. https://doi.org/10.1016/S0030-5898(20)30487-2
15. Su, K.-C., Yen, Y.-C., Wang, C.-H., Wang, Y.-L., & Wang, S.-P. (2024). Biomechanical comparisons of F.E.R.I. techniques with different type of intramedullary screws fixation for Jones fractures. Frontiers in Bioengineering and Biotechnology, 12, 1389127. https://doi.org/10.3389/fbioe.2024.1389127
16. Liu, D. S., Snyder, B. D., & Mahan, S. T. (2024). Fracture nonunion and delayed union. Journal of the Pediatric Orthopaedic Society of North America, 7, 100058. https://doi.org/10.1016/j.jposna.2024.100058
17. Rikken, Q. G. H., Dahmen, J., Hagemeijer, N. C., Sierevelt, I. N., Kerkhofs, G. M. M. J., & DiGiovanni, C. W. (2021). Adequate union rates for the treatment of acute proximal fifth metatarsal fractures. Knee Surgery, Sports Traumatology, Arthroscopy, 29(4), 1284–1293. https://doi.org/10.1007/s00167-020-06072-8
18. Herterich, V., Baumbach, S. F., Kaiser, A., Böcker, W., & Polzer, H. (2021). Fifth metatarsal fracture—A systematic review of the treatment of fractures of the base of the fifth metatarsal bone. Deutsches Ärzteblatt International, 118(37), 587–594. https://doi.org/10.3238/arztebl.m2021.0231
19. Kim, J. E., Lee, J.-Y., & Lee, G.-W. (2024). Proximal fifth metatarsal fractures: An up-to-date review. Arthroscopy, Orthopaedics, and Sports Medicine, 11(2), 49–56. https://doi.org/10.14517/aosm24012
20. Balu, A.R.; Baumann, A.N.; Burkhead, D.; Talaski, G.M.; Anastasio, A.T.; Walley, K.C.; & Adams, S.B. (2024). Assessing the Biomechanical, Kinematic, and Force Distribution Properties of the Foot Following Tarsometatarsal Joint Arthrodesis: A Systematic Review. Applied Sciences, 14, 765. https://doi.org/10.3390/app14020765
21. Physiopedia. (n.d.). Metatarsus adductus. Retrieved August 31, 2025, from https://www.physio-pedia.com/Metatarsus_Adductusowl.purdue.edu+7physio-pedia.com+7physio-pedia.com+7
22. Physiopedia/The Codman Group. (n.d.). Metatarsal fractures. In OrthoPaedia. Retrieved August 31, 2025, from https://www.orthopaedia.com/metatarsal-fractures/
23. Huh, J., & Easley, M. E. (n.d.). Surgical management of proximal fifth metatarsal fractures. In Musculoskeletal Key. Retrieved August 31, 2025, from https://musculoskeletalkey.com/surgical-management-of-proximal-fifth-metatarsal-fractures/ Musculoskeletal Key+2Musculoskeletal Key+2Jucm+12Musculoskeletal Key+12Musculoskeletal Key+12
24. Parekh, Shah. Optimal Time to Return to Play and Performance After Jones Fracture Surgery in the National Football League. Foot & Ankle Orthopaedics, 2(3). https://journals.sagepub.com/doi/10.1177/2473011417S000068
Injury Care Solutions Group (ICSG) provides educational expert content that does not constitute medical advice, diagnosis, treatment, or legal advice or solicitation. ICSG is not a law firm or medical provider. Use of this website does not create a doctor–patient or attorney–client relationship. Do not send PHI through this Website. Attorney references (including references to Ben Martin Law Group) are for convenience only, and are not endorsements, guarantees or attorney advertising. Past results do not predict future outcomes. See Full Disclaimer and Privacy Policy. If deemed attorney advertising: Ben C. Martin, 4500 Maple Ave., Suite 400, Dallas, Texas 75219, licensed by the State Bar of Texas and Pennsylvania.