Authored by:
Greg Vigna, MD; JD; Adam Suchecki, Orthopedic PA, CLCP;
Vanessa Young, OTR/L, CLCP; Elizabeth German, DPT
Introduction:
“Midfoot injuries are rare and account for about 5% of all foot injuries. Among these, fracture- dislocation of the Chopart and Lisfrac joints is the most common.” (6) Of clinical importance, it should be mentioned that Lisfranc injuries occur most frequently in the third decade of life, with injuries being 2-4x more likely in men than women. (16) Lisfranc fractures are notably named after a French surgeon in the Napoleonic era, Jacques Lisfranc de St. Martin, who was the first to describe injuries and amputations at this level of the foot. (16) This specific type of injury occurred when a soldier fell from his horse, with his foot getting stuck in the stirrup, leading to a severe midfoot injury and a fracture-dislocation at the tarsometatarsal joint complex.
The midfoot is composed of 5 tarsal bones: the navicular, cuboid, and three cuneiform bones (medial, intermediate and lateral). This region connects the hindfoot (heel/ankle) to the forefoot (toes). The Lisfranc joint complex, also known as the tarsometatarsal (TMT) joint, is formed where the midfoot bones meet the metatarsals, as well as the dorsal ligaments, plantar ligaments, and interosseous ligaments, that serve to stabilize the joint. Although the joint complex consists of a number of articulations and ligaments, the “Lisfranc ligament” itself, is found at the articulation between the medial cuneiform and the medial base of the second metatarsal, and is also known as the oblique interosseous ligament. (4)
The Lisfranc joint performs two main functions:
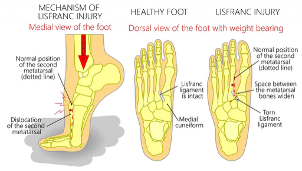
Figure courtesy of “Lisfranc injury,” Campbell Clinic Orthopaedics (n.d.). (22)
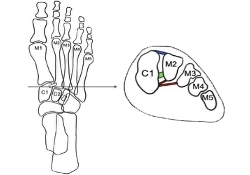
Figure courtesy of Brisbane Physiotherapy & Podiatry (n.d.). (23)
Note: The transverse arch forms between the cuneiforms, cuboid and metatarsals. This arch helps support the foot and provide stability during weight bearing. (16)
The Lisfranc joint can be subdivided into 3 key zones: the medial, middle, and lateral columns. And injury to each of these zones may require significantly different treatment options. (14)
The 3 zones are:
The important thing to note is that each zone is responsible for a finite amount of movement and performs distinct functional patterns of movement. The medial and middle columns allow small motion at the joints (3.5mm in the coronal and 0.6mm in the sagittal plane), whereas the lateral column allows for increased movement (up to 13mm in the sagittal plane). This comes into play as the lateral column functions as a shock absorber on uneven surfaces with gait, thus making it an important area to maintain mobility, if at all possible, with treatment of Lisfranc injuries.
Understanding the joint-specific mobility of the area, helps to appreciate the functions of the midfoot, which are:
Injury to the Lisfranc complex leads to unstable joints and uneven transfer of force from the midfoot to/from the forefoot. This may further lead to collapse of the transverse arch of the foot, gait abnormalities, and osteoarthritis. (14)
A Lisfranc injury can encompass a wide array of possibilities, from simple ligamentous subluxations/sprains to unstable open fractures and dislocations, leading to significant soft tissue injury. “Occurrences of TMT injuries are rare, accounting for approximately 0.2% of all fractures.” (13)
Forces Causing Injury:
Lisfranc injuries are generally classified in two ways:
In a study performed by Mahesh, M. et al., it was found that “the most common cause of injury was road traffic accidents (50%), followed by falls from height (20%), accidental falls (16.67%), crush and twisting injuries (6.67%). This trend reflects the high-energy nature of these injuries.” (3)
Patient Presentation (Symptoms and Physical Findings):
Patients tend to present with symptoms including:
A thorough clinical and physical examination is required when assessing the midfoot for a possible Lisfranc injury. Through questioning it is important to ascertain the exact mechanism of injury, including foot position during injury, direction of force, and the amount of energy involved. (16) Along with the physical signs described above, it is important to assess joint position and to complete: a stress test, piano key tests, and an assessment for pain/instability with passive motion of the midfoot into abduction while stabilizing the tarsometatarsal joints. (13) Based on these findings, the physician will determine what diagnostic imaging is indicated.
In an article by Siddiqui, et al. it was found that “An estimated 20% of all Lisfranc injuries are initially undiagnosed clinically, which could reflect their subtle initial presentation or the fact that they may occur with polytrauma and may be overlooked while other critical injuries are being addressed… when Lisfranc injuries are missed or undertreated, they can lead to significant midfoot instability, planovalgus deformity, and osteoarthritis.” (18)
Diagnostic Testing:
Imaging generally begins with radiographs, including anteroposterior, lateral, and medial oblique views. “Standard 3 view radiographs of the foot are recommended initially to assess for bony injuries, such as the ‘fleck sign’ from an avulsion of the Lisfranc ligament”. (4) A disadvantage to radiograph imaging is that it is unable to show ligamentous subluxations or subtle injuries. This can, at times, lead to delayed treatment, prolonged pain, post-traumatic arthritis and flat foot deformity.
Dependent on the results of the radiographic imaging and the physical examination, the physician may order further testing, including:
“Despite advances in diagnostic techniques and treatment modalities, Lisfranc injuries remain frequently misdiagnosed or inadequately managed, contributing to poor functional outcomes”. (3) A Lisfranc injury is a radiographically “smaller” injury, but it has been found that, “even 1mm displacement of the second metatarsal base reduces the tarsometatarsal contact area by 13.1%.” (2)
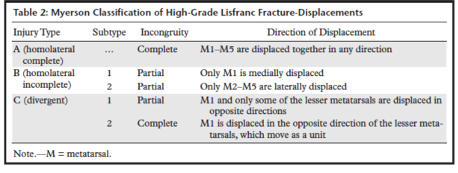
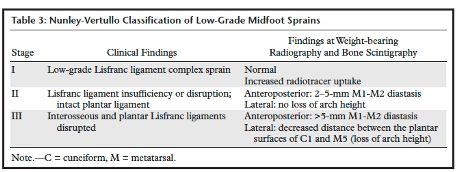
The Myerson classification system is the most widely accepted classification, and is utilized with high-impact injuries, to describe Lisfranc injuries based on the pattern of disruption. For low-impact injuries, the Nunley and Vertullo classification based on clinical findings, was developed, by comparative weight bearing radiographs, and bone scintigraphy. (18) These varying classification systems allow physicians to more accurately diagnose and begin appropriate treatment.
Below are depictions of both the Myerson and Nunly-Vertullo classification systems provided from an article published by Siddiqui, et. al. (18)
Surgical and Non-Surgical Treatment of Lisfranc Injuries:
As with any injury, both conservative and surgical treatment options must be evaluated and considered and are dependent on the type of injury. “In accordance with the recent literature the current trend is non-surgical treatment for undisplaced injuries, whilst all injuries that show load instability or diastasis of the TMT joints required surgical treatment with anatomical reduction and internal fixation”. (16) No matter if surgical or non-surgical treatment is pursued, the overarching goals remain the same: restore stability, minimize long-term complications, and recover normal foot function and mobility.
Conservative (non-surgical) treatment is utilized for Lisfranc injuries including ligament sprains or non-displaced intra-articular fractures, that are stable during weight bearing. Treatment includes immobilization (in a cast/splint), serial radiographs to assess healing, and non-weight bearing status x 4-8 weeks, per physician preference. Following this period of time, progressive weight bearing will be added, along with a physical therapy to improve function and decrease pain via modalities, stretching and strengthening exercises.
Surgical intervention is required in unstable Lisfranc injuries. The primary goals of surgery is restoration of the anatomical alignment of the midfoot, improvement of load-bearing function, and decreased risk for development of osteoarthritis. It was found that “early surgical intervention tailored to injury type is crucial for optimal recovery and minimizing long-term complications”. (3)
The types of surgery currently available to treat Lisfranc injuries are:
Types of ORIF include:
In the past, “arthrodesis was reserved as a salvage procedure for patients with failed ORIF or who developed post-traumatic OA, though, over the past decade, primary arthrodesis has been increasingly used as an initial treatment option…Primary arthrodesis serves as a particularly good option for highly comminuted, unstable injuries due to bone loss and high reoperation rates with ORIF”. (4) In a study by Sun, C. et al, it was found that “PA (primary arthrodesis) of the first TMT joint provided a better medium-term outcome than ORIF for Lisfranc injuries with the first TMT dislocation. PA prevented redislocation, pain, and revision as well”. (5)
Rehabilitation Required:
Regardless of surgical or non-surgical treatment, the primary goal is to decrease pain and improve foot stability. Physical therapy is often recommended to address these concerns. Physical therapists will work with physicians who provide guidelines based on the quality of fixation, quality of the bone, and the healing of the fracture.
Physical therapists use this information to provide an individualized approach to rehabilitation based on the fracture type, healing progress, and overall condition of the patient. Physical therapy generally follows similar principles and phases for recovery, with varying degrees of implementation based on injury and clinical discretion. The phases include:
The physician works closely with the physical therapist to provide guidelines for weight bearing and progression through these stages.
Home Modifications:
Following a Lisfranc fracture-dislocation, especially if requiring surgical intervention, adjustments in the home environment are often necessary. In the early recovery phase, these changes help ensure safety, reduce the risk of falls, and make daily activities more manageable. Over the long term, modifications can also support independence in the case that pain, dysfunctions of mobility, or additional surgeries occur. A meta-analysis by Stark, Keglovits, Arbesman, and Lieberman (2017) found strong evidence that home modification interventions improve function and reduce both the rate and risk of falls in community dwelling adults. (22)
Postoperative Modifications:
Short-term needs include supporting reduced weight-bearing, maintaining ADL participation, and preventing re-injury. Mobility devices could include, knee scooter, crutches, walker, cane, CAM boot, and post-operative brace/s. Bathroom safety can be addressed with a shower chair, handheld shower head, raised toilet seat with arms, and wound protection. Adaptive equipment may include a bedside commode, item carriers, and mobility aids such as knee scooters, walkers, or crutches. Client-centered modifications may involve portable ramps or threshold adjustments, grab bars and handrails, and the option to set up living space on one floor or install a stair lift.
Long-Term Modifications:
Permanent changes promote safety, independence, and mobility. These may include fixed grab bars in high-use areas, raised laundry baskets, anti-fatigue mats for prolonged standing, and supportive footwear to reduce joint stress. Community mobility devices, such as a power scooter with lift may be necessary as one ages. Adjustable beds can aid rest and assist with leg elevation, while recliners with or without lift functions support edema management, transfers, and independence as mobility declines with age.
Early Complications:
A few complications to monitor early on in recovery, and throughout the first 1-2 years, include: midfoot instability with the loss of the transverse arch, joint stiffness, and delayed healing due to poor ligamentous blood supply.
Specific additional complications following surgical interventions include:[1]
Future Complications:
Long-term complications are not uncommon with Lisfranc injuries. In part, this may be due to difficulty in early detection and diagnosis of these fractures. “Neglected Lisfranc fractures cause post-traumatic arthritis and chronic foot pain which causes significant morbidity.” (2)
A few long-term complications to keep in mind following Lisfranc injuries include:
Of these complications, the most researched involves post-traumatic OA. A study by “Mulier et al. followed 30 months after ORIF for Lisfranc injuries and reported 94% of TMT joints had degeneration and arthritis.” (5)
Treatment for osteoarthritis can vary from conservative treatment to surgical procedures. Initially, conservative treatment may consist of trialing steroid injections in the painful joints, and orthotics to assist with foot positioning. The specific orthotics or footwear recommended should be individualized in consideration, but generally includes shoes with a wide toe box, flexible top surface, and rocker bottom sole to absorb shock during gait. Joint salvaging procedures may then be utilized in an attempt to decrease pain and improve function. These joint salvage procedures could include debridements and osteophyte removal, joint interposition of the soft-tissue, and placement of synthetic ceramic spherical joint spacers. If these procedures are unsuccessful in decreasing pain and/or improving function, a joint arthrodesis (fusion) may be considered. (12)
Lisfranc injuries may be “smaller” injuries on radiograph, but their effects and potential complications are impactful on a patient’s quality of life. Early detection and treatment is crucial in returning a patient to pain free, pre-injury, activity levels. Treatment should be individualized, and varies based on the exact location of injury, types of forces causing the injury, and resultant injury pattern. An individualized approach in regard to treatment, leads to the best potential outcomes for improved function, while also decreasing pain and risk of long-term complications.
A 45-year-old female, an avid recreational runner and office administrator, sustained an injury after tripping on an uneven step at a restaurant, in a hallway with insufficient lighting. She sustained an injury that involved twisting of her left ankle. She experienced immediate midfoot pain, swelling, and difficulty bearing weight. Initial evaluation at an urgent care center resulted in a diagnosis of a “foot sprain,” and she was advised to rest and use supportive footwear.
Over the next six weeks, her symptoms persisted with worsening midfoot pain, swelling, and difficulty walking, particularly when climbing stairs or standing for extended periods. She returned for reevaluation and was referred to an orthopedic specialist. Imaging, including radiographs and CT, revealed a Lisfranc (midfoot) fracture-dislocation with evidence of diastasis and early post-traumatic changes due to delayed treatment.
Given the instability and malalignment, surgical intervention was required. She underwent open reduction and internal fixation (ORIF) of the tarsometatarsal joint. Postoperatively, she was non-weight bearing for 8 weeks, followed by gradual rehabilitation. Despite adherence to therapy, she continues to experience residual midfoot stiffness, pain with prolonged walking, and intermittent swelling.
At her one-year follow-up, she reports difficulty returning to her previous level of running and fitness activities, as well as challenges wearing regular footwear. She expresses frustration and emotional distress related to her limited activity and lifestyle changes. She has been started on low-dose antidepressants and referred to counseling to support her coping.
These ongoing symptoms place her at risk for post-traumatic sequelae, including midfoot arthritis and chronic pain syndromes. Literature indicates that delayed recognition and treatment of Lisfranc injuries are associated with higher rates of residual dysfunction and early degenerative changes. Given her age, activity level, and the complexity of the injury, future surgical needs could include hardware removal or midfoot fusion if pain and degeneration progress.
Life Care Plan Considerations:
Medical Follow-up:
Modalities:
Diagnostic:
Pain Management:
Orthotics and Support:
Work and Functional Needs:
Durable Medical Equipment with replacement until life expectancy:
Home Care Needs:
Note: With each surgical procedure comes preoperative clearance visit/s, post-operative pain medications, possible blood thinners (if indicated), post-operative outpatient physical therapy, home health considerations for PT/OT/RN in the acute healing phase, attendant care for 2-6 weeks depending on procedure, bracing/orthotic needs, and DME.
Reference List
1. Riquet, P., & Baylac, P. (2023). Metatarsal fracture without lisfranc injury. Orthopaedics and Traumatology: Surgery and Research. 111. https://doi.org/10.1016/j.otsr.2024.104059
2. Akinyoola, A. L., Adegbehingbe, O. O., & Odunsi, A. O. (2011). Neglected divergent dislocation of the tarsometatarsal joint (Lisfranc injury): A case report. The Foot and Ankle Online Journal, 4(8), 1–5. https://doi.org/10.3827/faoj.2011.0408.0004
3. Mahesh, M., Madhavi, K., & Shantan Kumar, G. (2024). Functional and clinical outcomes of lisfranc injuries of foot: a comparative study of surgical and conservative management approaches. International Journal of Academic Medicine and Pharmacy, 6 (6), 309-313. https://doi.org/10.47009/jamp.2024.6.6.60
4. Saha, P., Smith, M. and Hasan, K. (2023) Treatment and Hardware Removal after Lisfranc Injury: A Narrative Review. Open Journal of Orthopedics , 13, 501-508. https://doi.org/10.4236/ojo.2023.1312049
5. Sun, C., Miao, X., Zhang, M., Yang, Y., Zhao, H., Tang, X., & Yu, G. (2022). Lisfranc injuries with dislocation the first tarsometatarsal joint: Primary arthrodesis or internal fixation (a randomized controlled trial). International Orthopaedics, 46(12), 2797–2807. https://doi.org/10.1007/s00264-022-05478-y
6. Alayed, I. (2021) Combined midfoot dislocation involving the naviculocuneiform and calcaneocuboid joints: a case report. The Egyptian Journal of Hospital Medicine, 83, 1017-1021. https://ejhm.journals.ekb.eg/ (???DOI???)
7. Sun, C., Miao, X., Zhang, M., Yang, Y., Zhao, H., Tang, X., & Yu, G. (2022). Lisfranc injuries with dislocation the first tarsometatarsal joint: Primary arthrodesis or internal fixation (a randomized controlled trial). International Orthopaedics, 46(12), 2797–2807. https://doi.org/10.1007/s00264-022-05478-y
8. Swords, M., & Schepers, T. (2025). Post traumatic complications after navicular fractures. Foot Ankle Clinic of North America, 30(1), 127-140. http://doi.org/10.1016/j.fcl.2024.06.010
9. Giaretta S, Aprato A, Anselmi A, et al. (2022). Acute navicular fractures: report of two cases and review of the literature. Lo Scalpello Journal, 36:172-178. https://doi.org/10.36149/0390-5276-269
10. K. Bagheri, A.T. Anastasio, E. Poehlein et al. (2023). Outcomes after total ankle arthroplasty with an average follow-up of 10 years: A systematic review and meta-analysis. Foot and Ankle Surgery. https://doi.org/10.1016/j.fas.2023.09.007
11. Watts, D., Moosa, A., Elahi, Z., Palmar, A., & Rodriguez-Merchan, E.C. (2022). Comparing the results of total ankle arthroplasty vs tibiotalar fusion (ankle arthrodesis) in patients with ankle osteoarthritis since 2006 to 2020: a systematic review. The Archives of Bone and Joint Surgery, 10(6): 470-479. https://doi.org/10.22038/ABJS.2021.55790.2778
12. Kane, B., Inocco, K., & Costa, A. (2023). Arthrodesis of the fourth and firth tarsometatarsal joints in a sensate patient with post-traumatic arthritis: a case report and surgical technique. Journal of the American Podiatric Medical Association, 113(2). https://pubmed.ncbi.nlm.nih.gov/37134056/
13. A. Chafik, S. Auhmani, F. Rifki, M. Akhouayri, B. Slioui, S. Bellasri, N. Hammoune, H. Doulhousne, A. Mouhcine. (2024). Lisfranc Injury: A Case Report and Literature Review. Scholars Journal of Medical Case Reports, 12(9): 1551-1554. https://doi.org/10.36347/sjmcr.2024.v12i09.011
14. Balu, A.R.; Baumann, A.N.; Burkhead, D.; Talaski, G.M.; Anastasio, A.T.; Walley, K.C.; & Adams, S.B. (2024). Assessing the Biomechanical, Kinematic, and Force Distribution Properties of the Foot Following Tarsometatarsal Joint Arthrodesis: A Systematic Review. Applied Sciences, 14, 765. https://doi.org/10.3390/app14020765
15. https://james-mccormack.com/advice-centre/lisfranc-injury/
16. Mascio, A., Greco, T., Maccauro, G., & Perisano, C. (2022). Lisfranc complex injuries management and treatment: Current knowledge. International Journal of Physiology, Pathophysiology and Pharmacology, 14(3), 161–170. http://www.ijppp.org
17. Buchanan, B. K., & Donnally, C. J., III. (2025). Lisfranc dislocation. In StatPearls [Internet]. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK448147/
18. Siddiqui, N.A., Galizia, M.S., Almusa, E., & Omar, I.M. (2014). Evaluation of the tarsometatarsal joint using conventional radiography, CT, and MR imaging. Radiographics of Radiological Society of North America, 34, 514-531. https://doi.org/10.1148/rg.342125215
19. Grewal, U.S., Onubogu, K., Southgate, C., & Dhinsa, B.S. (2020). Lisfranc injury: a review and simplified treatment algorithm. The Foot, 45. https://doi.org/10.1016/j.foot.2020.101719
20. Webster, Z., & Taylor, J. (2023). Post-operative Lisfranc injury: Clinical practice guideline. The Ohio State University Wexner Medical Center. https://tco.osu.edu
21. Singh, A., Lokikere, N., Saraogi, A., Unnikrishnan, P.N., & Davenport, J. (2020). Missed Lisfranc injuries – surgical vs conservative treatment. Irish Journal of Medical Science, 190: 653-656. https://doi.org/10.1007/s11845-020-02364-7
22. Stark, S., Keglovits, M., Arbesman, M., & Lieberman, D. (2017). Effect of home modification interventions on the participation of community-dwelling adults with health conditions: A systematic review. The American Journal of Occupational Therapy, 71(2), 7102290010p1–7102290010p11. https://pubmed.ncbi.nlm.nih.gov/28218595/
23. Brisbane Physiotherapy & Podiatry. (n.d.). Lisfranc injuries and physiotherapy management. Retrieved August 24, 2025, from URL
Injury Care Solutions Group (ICSG) provides educational expert content that does not constitute medical advice, diagnosis, treatment, or legal advice or solicitation. ICSG is not a law firm or medical provider. Use of this website does not create a doctor–patient or attorney–client relationship. Do not send PHI through this Website. Attorney references (including references to Ben Martin Law Group) are for convenience only, and are not endorsements, guarantees or attorney advertising. Past results do not predict future outcomes. See Full Disclaimer and Privacy Policy. If deemed attorney advertising: Ben C. Martin, 4500 Maple Ave., Suite 400, Dallas, Texas 75219, licensed by the State Bar of Texas and Pennsylvania.