Authored by:
Greg Vigna, MD, JD; Adam Suchecki, Orthopedic PA, CLCP;
Vanessa Young, OTR/L, CLCP; Elizabeth German, DPT
Introduction:
The Maisonneuve fracture is a unique and complicated injury of the lower leg, which can have debilitating outcomes if not treated appropriately. This specific fracture pattern was first described in 1840 through cadaveric studies by the French surgeon Jules Germain Francois Maisonneuve. It involves a proximal fibular fracture, along with a rupture of the tibiofibular syndesmosis and the anterior fibers of the deltoid ligament (1, 3). This injury is relatively rare, accounting for approximately 7% of all ankle fractures, and 5% of the ankle fractures that are treated surgically (3, 7, 14).
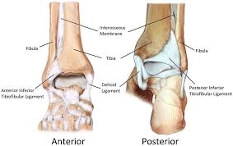
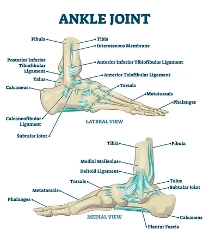
To grasp the complexity of this injury, one must understand the anatomy of the lower leg. The ankle joint consists of three bones. These include the distal tibia (medial malleolus), distal fibula (lateral malleolus), and the talus. Between the bones of the tibia and fibula, lies an interosseous membrane (IOM). And surrounding the joint is a vast array of ligaments providing stabilization. The ligamentous structures can be divided broadly into medial and lateral ligaments. The medial structure consists of the deltoid ligament, a large ligament that provides the main aspect of stability to the ankle (13). The lateral ligaments include the anterior talofibular ligament (ATFL), posterior talofibular ligament (PTFL), anterior inferior tibiofibular ligament (AITFL), and the calcaneofibular ligament (CFL). The term “tibiofibular syndesmosis” specifically refers to the ligamentous structure consisting of the AITFL, the PITFL, and the interosseous ligament, which, as a unit, plays an essential role in ankle function and stability (19, 26). The ankle joint functions to provide stability, while also adapting to various surfaces by allowing for inversion, eversion, plantar flexion and dorsiflexion movements. If disrupted, an individual will experience instability in their gait, along with pain, and have increased potential to develop early osteoarthritis (3).
(31)
(30)
Maisonneuve fractures are unique, in that an injury must encompass the following multifaceted pattern: (1, 2, 8, 9, 10, 12, 14, 17, 19, 28)
A Maisonneuve fracture has no single categorization technique, but instead relies on a combination of the Lauge-Hansen classification, the AO classification, and Weber classification systems (7, 13). The Lauge-Hansen addresses the forces causing injury, the AO classification describes the bone/location/type of fracture, and the Weber describes the location of fibular fracture. Altogether these classification systems provide a thorough description of the injury.
Forces Causing Injury:
In the research, “most authors conclude that the injury mechanism of Maisonneuve fracture is pronation-external rotation injury, belonging to stage III or IV pronation-external rotation mechanism according to Lauge-Hansen classification” (1, 6, 10). And while it is possible for this injury to occur via supination-external rotation forces, these are much less common than those involving pronation-external rotation forces.
The theorized sequence of events in a Maisonneuve fracture occurs in stages, beginning with a pronation-external rotation force, which leads to (1, 6, 10, 26):
A high-energy force is needed to create this injury. Therefore it is more commonly seen during traumatic sporting events, such as ice skating, cycling, running and dancing. However, it may also occur in falls down the stairs, tripping/slipping on the ground, falls from height, or motor vehicle accidents (7, 15).
Patient Presentation (Symptoms and Physical Findings):
“The Maisonneuve fracture is an uncommon fracture that can be easily overlooked in the evaluation of the traumatized ankle” (16). This is because the greatest amount of pain is usually localized surrounding the ankle joint itself, with relatively little pain in comparison throughout the fibula. A detailed patient history often reveals a twisting motion of the ankle and lower leg during injury.
Clinical presentation generally reveals severe ankle pain (worse with weight bearing); significant swelling and ecchymosis (bruising); restricted range of motion (ROM); ankle instability and feelings of “giving out”; difficulty walking with decreased push-off power; and tenderness at both the proximal fibula and the anterior inferior tibiofibular ligament (15, 17, 3, 9).
Clinical examination requires a thorough assessment of the lower extremities, especially the joints surrounding the ankle, including both the knee and foot. The physician typically evaluates both the injured and non-injured legs for comparison. Due to the injury location and significant edema often seen, inspection of the skin and palpation of neurovascular structures must be addressed, including assessment of the dorsalis pedis and posterior tibial pulses. A physical examination will include a multitude of tests completed by the physician, to include any, or all, of the following: Cotton test; Pronation-external rotation test; Squeeze test; Crossed-leg test; Valgus stress test (8, 6, 17, 19). In the case of surgery, the syndesmosis will be further evaluated within the procedure via the External rotation test &/or the Bone and hook test (23).
One of the biggest limitations in assessment of these injuries in the acute setting, is that due to significant pain and edema, these physical examinations/tests may lead to false positive results. In these cases, diagnostic imaging becomes even more valuable.
Diagnostic Testing:
Plain 3-view ankle radiographs are often the starting point of diagnostic testing in a Maisonneuve fracture. With diagnostic testing it is imperative to remember that due to the proximal nature of the fibular fracture location in these injuries, it is crucial to obtain X-rays of not only the ankle joint, but the knee as well for a comprehensive examination. Next, weight-bearing “stress” radiographs are frequently utilized to observe the syndesmosis for evaluation of injury stability. A Maisonneuve fracture is usually able to be diagnosed with a combination of clinical examination and plain radiographs (8, 6, 17, 19). These radiographs provide information on fibular fractures, fibular shortening, and any abnormal spacing between the tibia and fibula. In the event of preparing for surgical correction, an MRI &/or CT are often obtained for more precise planning. “Once Maisonneuve fracture is suspected, additional CT scans, stress X-ray, and MRI can help to determine the stability of the inferior tibiofibular syndesmosis and the integrity of the lateral collateral ligaments” (6).
Surgical and Non-Surgical Treatment:
The main goal in treatment for Maisonneuve fractures involves stabilization of the ankle joint following the syndesmotic lesion. Both surgical and conservative methods of treatment exist, however, the use of conservative treatment is quite rare in that a Maisonneuve fracture, in itself, is considered an “unstable injury”. In an article by Dietrich et. al, “It is admitted that a syndesmosis lesion may be associated with a significant instability of the joint, which could lead to osteoarthritis if not adequately stabilized… Nevertheless, some authors recommend conservative treatment of certain types of Maisonneuve fractures in cases of partial disruption of the syndesmosis, in the absence of diastasis, or in the absence of ligament or bone lesion of the medial malleolus” (8). Meaning that without rupture of the deltoid ligament, interosseous ligaments or medial malleoli fractures, and with correct positioning of the fibula maintained, these injuries can potentially be ruled “stable enough” for conservative treatment. Another instance that would require non-operative treatment may arise if the patient is a poor surgical candidate (3). In general, typical conservative treatment includes a short-leg walking cast x6 weeks, with partial weight-bearing and crutches.
Surgical correction is understood to be the primary method of treatment for Maisonneuve fractures, and in an article by Wang et al. it states, “To our knowledge, currently, once a Maisonneuve fracture is diagnosed, the operation is always recommended for fear of sequelae of inaccurate reconstruction of the articulation” (6). Due to the inherent instability of these fractures, surgery is recommended to: recover the anatomical morphology and accurate alignment of the ankle, and to reconstruct the stability of the ankle joint (6, 12, 14). “Treatment is generally surgical fixation with ORIF (open reduction internal fixation), but debate remains as to what type of syndesmotic fixation is most efficacious” (13). The goals for surgical treatment include (7, 20):
While surgical intervention is a definitive form of treatment for ankle instability at the lower tibiofibular syndesmosis, the treating physician may, or may not, choose to directly stabilize the proximal fibular fracture as well. This is because the physician is frequently able to stabilize the proximal fracture indirectly through fixation of the distal fibula to the tibia using trans-syndesmotic screws (3). It is believed that “while lateral plating of distal fibular fractures is often required to restore length and syndesmosis alignment, Maisonneuve fractures involving the proximal third of the fibula are generally treated with sydesmotic-only fixation. Anatomic alignment of the mortise can often be achieved through closed reduction of the fibula, and lateral plating proximally would require dissection of the peroneal nerve” (19). Fibular length and position plays a key role in ankle stabilization and its correction to neutral position is vital. Dattani et al., emphasized the importance of correcting the fibular length and external rotation in biomechanical studies. He states “The outward movement of the talus by 1mm reduced the tibial contact area by 42%. Reconstructing the tibiofibular space, restoring the length of the fibula, and stabilizing the position of the fibula in the tibial notch are important to maintain ankle stability, restore normal ankle biomechanics, and obtain a good prognosis” (14).
Restoration and stabilization of the ankle mortise and tibiofibular syndesmosis can occur in one of two ways. “Currently, the commonly used fixation methods for lower tibiofibular joint injury are strong (rigid) fixation and elastic fixation” (2, 7). An open reduction internal fixation (ORIF) or percutaneous technique may be used to achieve these corrections.
“Once syndesmotic stabilization is accomplished, an uneventful recovery is typical for this injury. Immobilization is employed for 1-3 weeks, followed by rehabilitation of the periarticular musculature. Weight bearing is delayed for 6-8 weeks, until syndesmotic screw removal” (11).
Rehabilitation Required:
Maisonneuve fractures are complex injuries, and treatment protocols can follow conservative or surgical approaches depending on the extent of injury. Rehabilitation protocols should be individualized, with physician guidance, to optimize functional outcomes. A physical therapist will assist in guiding the patient through the recovery process. Rehabilitation is typically tailored based on the type and severity of the fracture, the treatment approach and protocol established by the treating orthopedic physician, and the patient’s initial functional status and personal goals.
Physical therapy for Maisonneuve fractures generally follows consistent principles and phases of recovery, with varying degrees of implementation based on injury and clinical discretion. The phases include:
Home Modifications:
Following Maisonneuve injury, whether managed surgically or non-surgically, adjustments to the home environment are often necessary. In the early recovery phase, these changes promote safety, reduce fall risk, and make daily activities more manageable. Over the long term, home modifications can also support independence if pain, mobility limitations, or additional surgeries arise. A meta-analysis by Stark, Keglovits, Arbesman, and Lieberman (2017) found strong evidence that home modification interventions improve function and reduce both the rate and risk of falls in community dwelling adults (29).
Postoperative/Short-Term Modifications:
Short-term needs focus on supporting reduced weight-bearing, maintaining participation in ADLs (activities of daily living), and preventing re-injury. Bathroom safety can be addressed with the use of a shower chair, grab bars, a handheld shower head, and, when needed, a raised toilet seat with arms, along with appropriate wound protection during bathing. Adaptive equipment may include, depending on the individual, a bedside commode, item carriers, and mobility aids such as a wheelchair, walker, or crutches. Immobilization and stability devices, such as a short leg cast, a CAM boot, or other post-operative braces, should also be considered. Client-centered modifications may involve temporary portable ramps or threshold adjustments, additional grab bars and handrails, and the option to set up living space on one floor. Depending on the client’s age, strength, home set-up, and family dynamics, a temporary caregiver may be necessary for things such as meal preparation, driving, grocery acquisition, and deep cleaning.
Long-Term Modifications
If a patient experiences long-term complications such as osteoarthritis, heterotopic ossification, or malunion, permanent modifications may be needed to promote safety, independence, and mobility. These may include fixed grab bars in high-use areas, raised laundry baskets to reduce bending demands, anti-fatigue mats to improve comfort during prolonged standing, and supportive footwear to reduce joint stress and enhance stability.
Community mobility devices, such as a power scooter with a lift, may become necessary with advancing age or declining endurance. Adjustable beds can aid rest and assist with leg elevation, while recliners with or without lift functions support edema management, transfers, and independence as mobility declines with age.
Early Complications:
Maisonneuve fractures may be missed initially, leading to persistent pain and functional limitations. Two of the reasons for possible missed diagnosis include: 1) the fibula fracture is in the proximal aspect of the bone and a simple ankle X-ray will not capture it (a knee X-ray is needed as well), and 2) the superior fibular pain may be much less than that of the ankle joint and may be overshadowed causing it to be ignored by either the patient, physician, or both. “Therefore, in order to avoid the missed diagnosis when treating patients suffering from ankle injuries, it is recommended that the scope of the physical examination always extends to the distal and proximal joints near the injured part, considering injury forces can be transmitted along the axis of our limbs” (6).
“Moreover, Hintermann and Loren (in two separate findings) reported an incidence of cartilage lesions, including chondral defects and osteochondral lesions, in ankle fractures of 79.2%, respectively 63%. Yoshimura reported that all patients with MFC (Maisonneuve fracture complex), who underwent ankle arthroscopy, had cartilaginous damage to the medial section of the talar dome. Therefore, we started to treat patients with Maisonneuve fractures arthroscopically to detect and address concomitant injuries” (12). Benefits of utilizing ankle arthroscopy are that it can help detect and treat cartilage lesions of the talus and tibia, and be a guide fibular reduction as well.
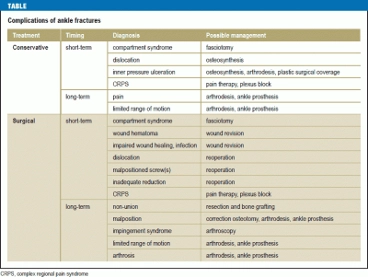
Complications that are more specifically associated with surgical repair include compartment syndrome (12, 26), infection (superficial or deep), deep vein thrombosis, loosening and failure of the internal fixation (14), delayed wound healing (19), possible perforation of the great saphenous vein, entrapment of the posterior tibial tendon, and soft tissue irritation (20). The most common reason for a reoperation is to provide symptomatic relief via hardware removal of syndesmotic screws. A summary of short and long term complications, as well as possible treatment options was presented in an article by Goost, et al. as follows.
(24)
Future Complications:
Without proper treatment and stabilization of the joint, an individual may experience long-term complications of post-traumatic osteoarthritis, chronic pain, heterotopic ossification, and permanent ankle instability (6, 12, 14, 21). “It is essential that the injury be recognized in the acute phase as the late sequelae of nonoperative management includes degenerative arthritis and pain, leading to a dysfunctional ankle” (11). Arthritis at the ankle joint may initially be treated with analgesics, orthotics and supportive shoes, but in later stages may require an arthrodesis surgery at the joint. With inadequate treatment, an individual may experience persistent tibiofibular diastasis and chronic pain, leading to functional limitations in daily activities, the ability to work, or sporting capabilities. Correct diagnosis and treatment thus proves critical in achieving both short and long-term optimal outcomes in patients following Maisonneuve fractures.
Patient Profile:
A 42 year old female recreational ice skater presented to the emergency department after sustaining a fall during skating practice. The patient reported losing her balance while her right foot was planted and externally rotated, resulting in a twisting injury to the ankle and lower leg. She immediately experienced severe pain in the right ankle and was unable to continue skating or walking. She denied direct trauma to the knee but noted vague discomfort along the upper portion of her lower leg.
On presentation, the patient ambulated with marked difficulty and required assistance. Examination of the right lower extremity revealed significant swelling and ecchymosis surrounding the ankle joint, with tenderness localized primarily to the medial ankle and anterior syndesmotic region. Active range of motion was severely limited due to pain, and the patient reported a sensation of ankle instability with attempted weight bearing.
Palpation revealed tenderness over the anterior inferior tibiofibular ligament and mild but notable tenderness over the proximal third of the fibula near the lateral aspect of the knee. Passive external rotation of the ankle reproduced pain. Neurovascular examination was normal.
Special tests were limited by pain and swelling, but included a positive squeeze test and pain reproduction with pronation–external rotation stress. Due to concern for syndesmotic injury, examination of the knee and proximal fibula was emphasized.
Initial three-view ankle radiographs demonstrated widening of the medial clear space and lateral clear space, raising concern for syndesmotic disruption. No obvious distal fibular fracture was visualized. Given the clinical suspicion for a Maisonneuve fracture, radiographs of the knee and entire tibia-fibula were obtained, revealing a spiral fracture of the proximal third of the fibula.
Stress radiographs confirmed instability of the tibiofibular syndesmosis. A subsequent CT scan of the ankle was obtained for surgical planning and demonstrated disruption of the syndesmotic complex without significant posterior malleolar involvement. Based on clinical and imaging findings, a diagnosis of Maisonneuve fracture was made.
The patient underwent open reduction and internal fixation (ORIF) with stabilization of the distal tibiofibular syndesmosis using trans-syndesmotic screw fixation. The medial malleolar avulsion fracture was addressed intraoperatively, and anatomic alignment of the ankle mortise was restored. The proximal fibular fracture was not directly fixated, as adequate reduction was achieved through distal syndesmotic stabilization. Postoperatively, the patient was immobilized in a short-leg splint and maintained non–weight bearing status. Deep vein thrombosis prophylaxis was initiated due to prolonged immobilization.
Following surgery, the patient was transitioned to a CAM boot after two weeks. Early rehabilitation focused on edema management, pain control, and maintenance of proximal strength. Gentle ankle range of motion exercises were initiated once cleared by the orthopedic surgeon. At six weeks postoperatively, progressive weight bearing was introduced following removal of the syndesmotic screws. Physical therapy emphasized restoration of ankle range of motion, strengthening of the gastrocnemius-soleus complex, balance training, and gait re-education.
By three months, the patient ambulated independently in supportive footwear with minimal discomfort. At six months, she demonstrated near-normal ankle range of motion and strength, though she reported mild fatigue with prolonged standing. At one-year follow-up, the patient demonstrated a stable, pain-free gait and returned to modified recreational skating activity, with no reported episodes of ankle instability.
During the early recovery phase, the patient required temporary home modifications, including use of a shower chair, grab bars in the bathroom, and relocation of living activities to a single floor. She was instructed on safe use of crutches with weight-bearing progression.
Education focused on adherence to weight-bearing restrictions, gradual return to activity, proper footwear, and the importance of ongoing strengthening to reduce the risk of chronic instability and post-traumatic osteoarthritis. She was counseled on the risk of long-term complications and periodic orthopedic follow-up was recommended to monitor joint health.
Life Care Plan Considerations:
Note: Each surgical procedure comes with: preoperative clearance visit, post-operative pain medications, possible blood thinners (if indicated), post-operative outpatient physical therapy, home health considerations for PT/OT/RN in acute healing phase (if indicated), attendant care for 2-6 weeks depending on procedure (if indicated), bracing/orthotic needs, and DME.
Injury Care Solutions Group (ICSG) provides educational expert content that does not constitute medical advice, diagnosis, treatment, or legal advice or solicitation. ICSG is not a law firm or medical provider. Use of this website does not create a doctor–patient or attorney–client relationship. Do not send PHI through this Website. Attorney references (including references to Ben Martin Law Group) are for convenience only, and are not endorsements, guarantees or attorney advertising. Past results do not predict future outcomes. See Full Disclaimer and Privacy Policy. If deemed attorney advertising: Ben C. Martin, 4500 Maple Ave., Suite 400, Dallas, Texas 75219, licensed by the State Bar of Texas and Pennsylvania.