Authored by:
Greg Vigna, MD; JD; Adam Suchecki, Orthopedic PA, CLCP;
Vanessa Young, OTR/L, CLCP; Elizabeth German, DPT
Introduction:
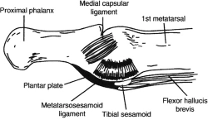
The first metatarsophalangeal (MTP) joint complex is a unique capsuloligamentous structure of the forefoot, providing stability to the great toe (hallux). It consists of the plantar plate, medial and lateral collateral ligaments, adductor and abductor hallucis tendons, and the medial and lateral heads of the flexor hallucis brevis tendon, surrounding embedded sesamoid bones. These two sesamoid bones (the tibial and fibular sesamoids) function as a fulcrum to increase leverage of the flexor hallucis brevis and longus muscles during the push-off phase of gait. The plantar plate itself is the structure that connects the metatarsal head to the base of the proximal phalanx, thus creating the first MTP joint. The joint functions as a hinge and sliding joint, and while there is little inherent bony stability within this joint, the capsuloligamentous soft tissue structures surrounding it provide the bulk of stability (4, 10). During normal gait, the first MTP joint must withstand 40-60% of an individual’s body weight. This increases to 2-3x an individual’s body weight during motor activity such as jogging, and up to 8x an individual’s body weight with sprinting or jumping. (1)
(6)
In the mid-1970s, the use of artificial turf began to be used in colleges and sports facilities, as a replacement to traditional grass fields, in order to decrease maintenance challenges. However, along this same time, Universities began to see increases in a unique subset of injuries to American footballers practicing on this first generation artificial turf. The injury was occurring at the plantar metatarsophalangeal-sesamoid complex of the great toe (the first metatarsophalangeal, MTP, joint). The injury involved a hyperextension force of the MTP joint injuring the surrounding plantar soft tissue structures. The term “turf toe” was initially coined by Dr. Bowers in 1976, and was described as a “sprain of the plantar capsule ligament of the great toe” (13). It is thought that the increased incidence of turf toe injuries at this time may have been due to both the introduction of lighter, more flexible shoes, and/or the changes in surface-cleat interaction with more rigid synthetic surfaces (1). Turf toe injuries were initially described according to the Clanton and Ford Classification. However, over time, this has evolved into the Anderson criteria, which is based on both physical exam and radiographic findings.
(17)

(6)
A further progression of first MTP joint injury, occurring with increased compression forces, is dislocation. In this instance, “most reported cases of dislocation of the great toe involve dislocation of the metatarsophalangeal (MTP) joint due to its greater mobility and longer level arm. Dislocation of the interphalangeal (IP) joint of the hallux is very rare, and when it does occur it is usually irreducible and dorsal. (2) ” Using the Jahss classification, these dorsal dislocations of the MTP are described based on the involvement of the sesamoid bones. “Type I is a dorsal dislocation of the MTP joint and sesamoid bone with rupture of the capsule; however, the intersesamoid ligament and the sesamoid bone remain intact. Type II dorsal dislocations are either associated with a disruption of the intersesamoid ligament (Type IIA) or involve a transverse fracture of either sesamoids (Type IIB). There is also a Type IIC classification that was proposed by Copeland et al., which represents a combination of both complete disruption of the intersesamoid ligament and a transverse fracture of either sesamoid.” (2)

(21)
Forces Causing Injury:
Both turf toe and dorsal dislocation of the great toe occur as the result of forces causing an axial load, onto a hyperextended MTP joint, with fixed equinus at the ankle. The compressive load drives the hallux MTP joint into hyperextension, leading to tension failure, and attenuation or disruption of the plantar capsular ligamentous complex surrounding the joint (1).
“Dorsal dislocation of the 1st and 2nd MTP joints combined is an infrequent yet clinically significant injury that primarily arises from traumatic incidents, such as crush injuries or direct impacts to the foot (11).” These types of injuries may occur in sports, motor vehicle accidents, falls, or crush injuries in occupational settings. And, “if unrecognized, can lead to chronic problems including: decreased push-off strength, persistent pain, progressive deformity, and eventual joint degeneration. (1)”
Patient Presentation (Symptoms and Physical Findings):
A clinician will complete a thorough and targeted history and physical examination. A patient’s history will generally be telling of a MTP hyperextension injury. They “may recall sustaining a compressive axial load while the ankle is plantar flexed and hallux extended” (1). The patient may complain of pain and stiffness, while showing weakness in the push-off (heel raised) phase of gait. Pain is generally described in the area distal to the sesamoid bones. Of clinical note, it is important to consider that complaints of pain proximal to the sesamoids generally indicates strain of the flexor hallucis brevis, and not a turf toe injury.
During examination the physician will assess the range of motion (ROM) of the MTP joint. Normal ROM includes 40-75 degrees dorsiflexion and 30-35 degrees of plantar flexion. The clinician will also assess for strength, edema, ecchymosis, and malalignment while palpating the dorsal capsule, plantar sesamoid complex, and collateral ligaments (1). Multidirectional stability testing of the first MTP joint is assessed with: AP translation, vertical Lachman’s test, and varus/valgus movements.
Diagnostic Testing:
Imaging is helpful to assess an injury, and its severity, within the MTP joint complex. It is preferred to compare imaging of both the injured and non-injured (contralateral) foot if able. Standard weightbearing AP and lateral sesamoid axial radiographs are needed, as well as non-weight bearing oblique views. A key factor to note, is that radiographs following a turf toe injury may appear normal if the injury has occurred solely to the capsuloligamentous complex. However, with fracture or dislocation of bony structures, evidence will be apparent in these radiographs. Additional radiograph imaging could include a forced dorsiflexion lateral view x-ray. This would be done to observe for any lack of distal migration of the sesamoid bones due to disruption of the plantar plate.
A fluoroscopy may be another beneficial technique used to observe for potential inability of the sesamoid bones to track distally with extension of the MTP. Additionally, an MRI may be a useful tool to evaluate plantar plate injuries with greater accuracy and determine the extent of the soft tissue injury.
Surgical and Non-Surgical Treatment:
Turf toe injuries tend to require non-surgical treatment. However in higher grade injuries or non-healing injuries, surgical intervention may be required. “There are several well-established indications for operative treatment of a turf toe injury. These may include large capsular avulsions, diastasis or a bipartite sesamoid, sesamoid fractures, retracted sesamoids, traumatic hallux valgus, vertical instability, loose bodies, chondral injury and failure of conservative treatment” (5, 14) However, “fewer than 2% of turf toe injuries require operative intervention” (1).
The time to return to sport following a turf toe injury depends on the severity of injury and the athlete’s level of competition and a common classification for the severithy of the plantar capsule disruption is the Anderson’s classification: 1) Grade I being less severe, involving stretch of the plantar complex with localized pain and swelling, 2) Grade II involve partial tear of the plantar capsule of the first MTP joint, and 3) Grade III are complete ruptures of the plantar plate. Grade I injuries require icing, taping, and an orthotic. Grade II injuries require a period of non-weightbearing and at least two weeks out of sports activity. Grade III injuries are complete ruptures of the plantar plate, and may require six months of no sports related activities and sometimes may require surgery.(25)
Dislocations of the great toe tend to follow a different trajectory, due to their likelihood of presenting in a continued dislocated (non-reduced) state. The initial focus is to attain reduction of the joint into a normal anatomical position. This can be accomplished via closed or open techniques based on the severity of injury. In general, the “invagination of the sesamoid-plantar plate complex into the interphalangeal space is the main reason for unsuccessful closed reduction attempts (11).” In this case, an open reduction, using percutaneous reduction may be necessary.
Non-surgical treatment interventions for either injury may include: rest, ice, analgesics, protected weight bearing (using crutches, knee scooter or walker) if pain prevents mobility; wearing a walking boot/stiff soled shoe with a turf toe plate insert (or custom orthotic with a Morton’s extension) to prevent further strain on the plantar ligament; and taping the hallux in a slightly plantar flexed position to provide rest to the ligament during healing. With difficult to treat cases, biologic therapies, such as platelet-rich plasma (PRP) injection or autologous conditioned plasma (ACP) injection, may be beneficial.
Rehabilitation Required:
Due to the variety in presentation of turf toe and great toe dislocation injuries, rehabilitation must be individualized to optimize patient outcomes. A physical therapist will assist in guiding the patient through the recovery process. There is not one set protocol, but instead the rehabilitation process will be tailored by: the type/severity of injury, the treatment approach and protocol of the orthopedic physician treating the patient, and the patient’s initial status and goals. (23)
Physical therapy generally follows similar principles and phases for recovery, with varying degrees of implementation based on injury and clinical discretion. The phases include:
Postoperative Modifications:
Short-term needs include supporting reduced weight-bearing (if indicated), maintaining ADL participation, and preventing re-injury. Mobility devices could include, knee scooter, crutches, walker, cane, CAM boot, and post-operative brace/s. Bathroom safety can be addressed with a shower chair, handheld shower head, raised toilet seat with arms, and wound protection. Adaptive equipment may include a bedside commode, item carriers, and mobility aids. Client-centered modifications may involve portable ramps or threshold adjustments, grab bars and handrails, and the option to set up living space on one floor or install a stair lift.
Long-Term Modifications
If a patient experiences long-term complications such as hallux rigidis or toe deformity leading to pain and decreased function, permanent changes should be considered to promote safety, independence, and mobility. These may include fixed grab bars in high-use areas, raised laundry baskets, anti-fatigue mats for prolonged standing, and supportive footwear to reduce joint stress. Community mobility devices, such as a power scooter with lift may be necessary as one ages. Adjustable beds can aid rest and assist with leg elevation, while recliners with or without lift functions support edema management, transfers, and independence as mobility declines with age.
Early Complications:
“Without proper treatment, the disruption of this complex (the first MTP joint) can create instability, dysfunction and ultimately deformity.” (10) Acute complications that may arise with closed or open reduction of dislocation include: incomplete reduction, soft tissue injury, fracture, joint stiffness and recurrent dislocation. Complications arising from open reduction procedures may include: infection, delayed healing, neurovascular injury, orthopedic hardware complication, wound healing issues, plantar nerve neuroma development, joint stiffness and adhesions (11).
Future Complications:
Long term delayed or incorrect treatment of turf toe, or dislocations, may lead to chronic pain, loss of push off strength, hallux rigidis and osteoarthritis, claw-toe or cock-up deformity, traumatic bunion deformity/progressive hallux valgus, loose bodies in the joint space, and joint fibrosis (4, 13). Additional potential complications include osteonecrosis of the metatarsal head, neuroalgodystrophy, and pseudarthrosis (11). Treatment of these longer term complications may involve: corticosteroid or hyaluronic acid injections, fasciotomy, tendon lengthening procedure, Girdleston-Taylor transfer, IP fusion for fixed contractures, and removal of bone spurs, osteotomy, arthroplasty or arthrodesis (fusion) in the case of hallux rigidus. (1)
Turf toe injury and great toe dislocations require prompt assessment and treatment in order to decrease the likelihood of developing late-sequelae issues and long-term complications. Successful outcomes can often be achieved through individualized care plans, monitored by a physician. Whether for a high level athlete attempting to return to sport, or an individual looking to continue their ability to complete ADLs, addressing and treating injuries to the first MTP joint is critical for successful long term management.
Patient Profile:
A 42 year old male warehouse worker sustained an injury to his right foot after slipping from a loading ramp while carrying a heavy box. He reported that as he attempted to regain balance, his right forefoot caught on the ramp surface while the ankle remained in plantar flexion, forcing the great toe into hyperextension. He immediately experienced sharp pain and noted an inability to move the toe. Swelling and ecchymosis developed rapidly over the dorsum of the first metatarsophalangeal (MTP) joint. The patient presented to the emergency department within two hours of injury, complaining of persistent pain and deformity at the base of the great toe, with inability to bear weight on the forefoot.
Physical examination revealed visible dorsal displacement of the proximal phalanx relative to the first metatarsal head, with plantar prominence of the metatarsal and blanching of the overlying skin. The patient exhibited significant edema, tenderness over the plantar aspect of the first MTP joint, and decreased range of motion. Neurovascular status was intact. Plain radiographs (AP, lateral, and sesamoid axial views) demonstrated a complete dorsal dislocation of the first MTP joint with the sesamoids remaining in their normal plantar position, consistent with a Jahss Type III dislocation pattern. No fracture lines were noted.
Closed reduction was provided under local anesthesia by way of axial traction with gentle plantar flexion of the proximal phalanx resulting in successful reduction of the joint, confirmed by post-reduction radiographs showing normal alignment of the metatarsal head and sesamoid complex. The toe was immobilized in a neutral to slightly plantar-flexed position using a postoperative shoe and compressive dressing.
The patient was advised to remain non-weightbearing for 2 weeks, progressing to partial weightbearing in a CAM boot for an additional 4 weeks. Analgesics and NSAIDs were prescribed for pain and inflammation management.
Following immobilization, the patient began physical therapy focused on gradual restoration of range of motion, strengthening of intrinsic and extrinsic foot muscles, and gait training. By 10 weeks post-injury, he was ambulating in supportive footwear with minimal pain and had regained near-normal motion of the MTP joint.
At the 3-month follow-up, the patient reported mild discomfort with prolonged standing but was able to perform full work duties without limitation. At 6 months post-injury, the patient demonstrated stable alignment and pain-free gait. He reported mild stiffness during toe-off phase of gait but denied recurrent dislocations. Long-term monitoring was recommended due to risk of degenerative joint changes and hallux rigidus associated with prior MTP joint trauma. Future care consideration would include:
Note: Each surgical procedure comes with: preoperative clearance visit, post-operative pain medications, possible blood thinners (if indicated), post-operative outpatient physical therapy, home health considerations for PT/OT/RN in acute healing phase (if indicated), attendant care for 2-6 weeks depending on procedure (if indicated), bracing/orthotic needs, and DME. Surgical considerations for advanced OA/hallux rigidus include:
Injury Care Solutions Group (ICSG) provides educational expert content that does not constitute medical advice, diagnosis, treatment, or legal advice or solicitation. ICSG is not a law firm or medical provider. Use of this website does not create a doctor–patient or attorney–client relationship. Do not send PHI through this Website. Attorney references (including references to Ben Martin Law Group) are for convenience only, and are not endorsements, guarantees or attorney advertising. Past results do not predict future outcomes. See Full Disclaimer and Privacy Policy. If deemed attorney advertising: Ben C. Martin, 4500 Maple Ave., Suite 400, Dallas, Texas 75219, licensed by the State Bar of Texas and Pennsylvania.